ChikDenZi - ArboWatch
Multi-source surveillance platform for critical Arboviruses

Arboviral Disease Dashboards
Chikungunya
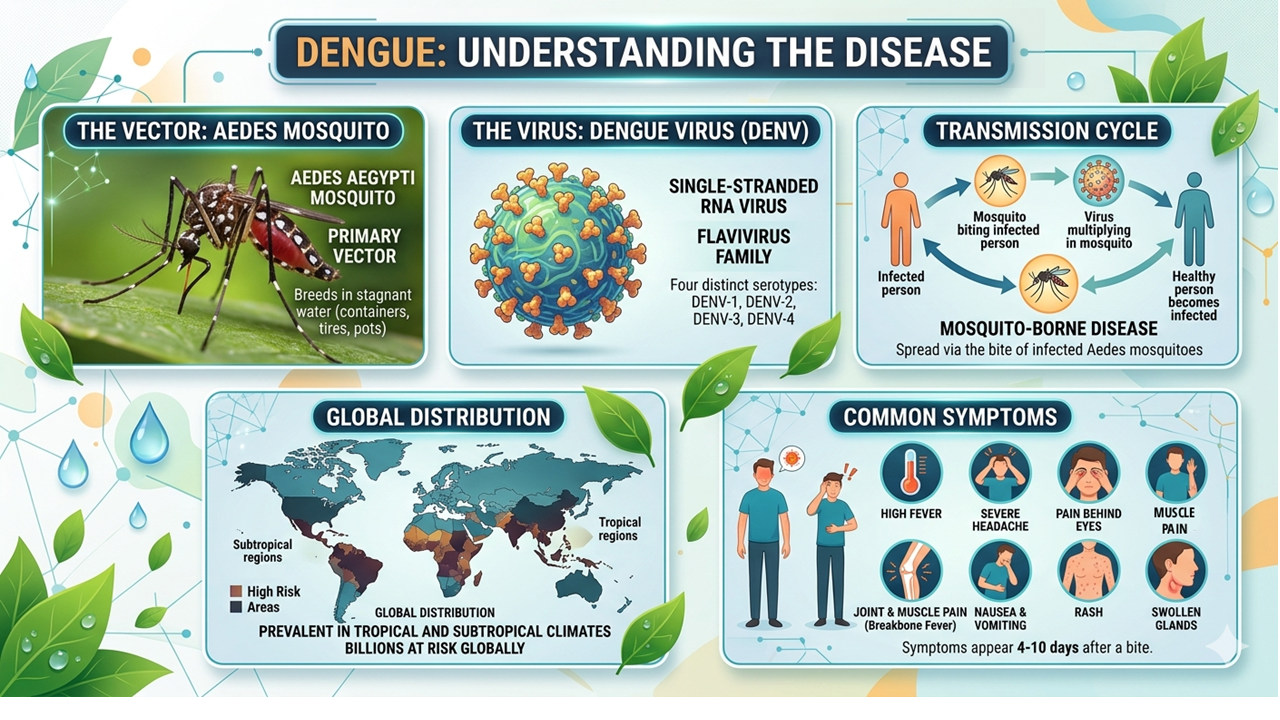
Dengue

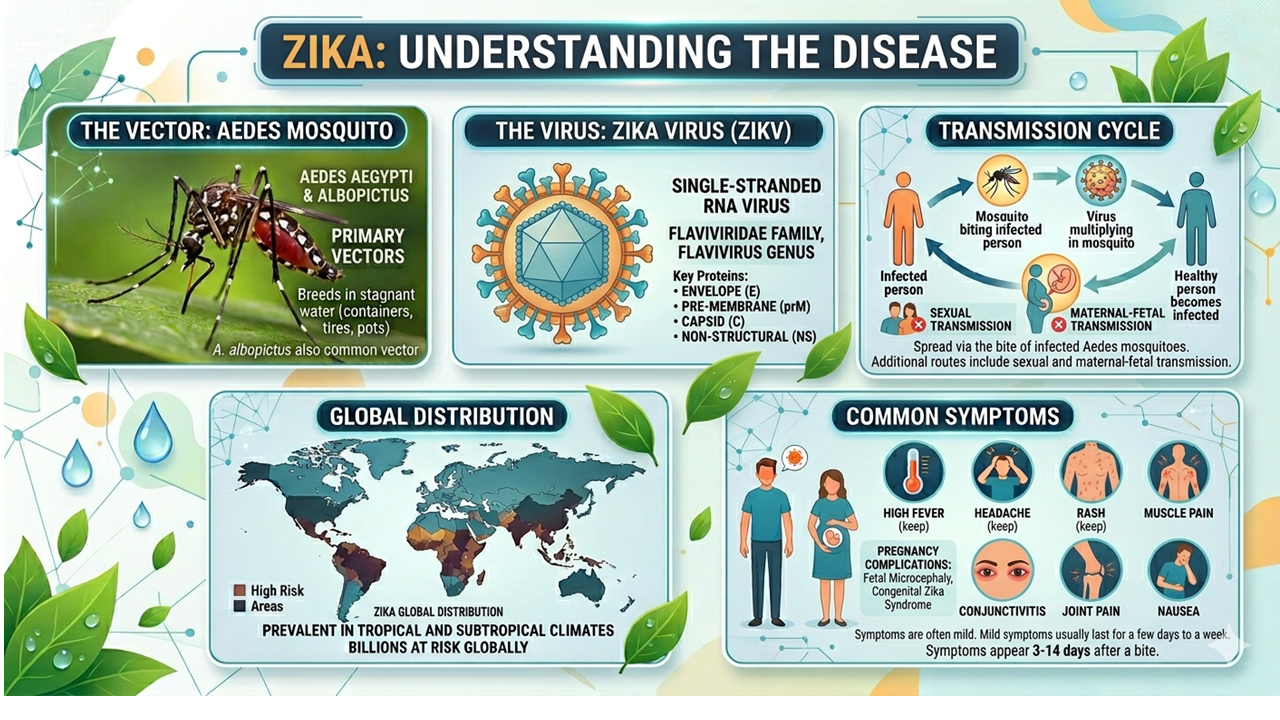
Zika
Overview
Published literature, mapping, and recent news tracked together in one view.
Interactive visualization of cumulative Chikungunya (2018-2025), Dengue(2019-2025), and Zika (2017-2024) cases reported across India.
About Us
Dr. Amit Sharma leads our research team at the International Centre for Genetic Engineering and Biotechnology (ICGEB), New Delhi. The lab brings together two collaborative research streams, united by a shared goal of addressing and understanding infectious diseases. The Structural Parasitology unit focuses on Plasmodium biology, mainly on molecular structures and pathways that play a crucial role in Malarial pathogenesis. Alongside, the Virus Research group explores the epidemiology and molecular mechanisms of Dengue, Chikungunya, and Zika viruses. Together, these multidisciplinary teams combine structural biology, molecular virology, and data-driven surveillance to advance public health and strengthen preparedness.
ChikDenZi Database represents a collaborative effort by our team members to enable real- time surveillance of vector-borne diseases such as Chikungunya, Dengue, and Zika. The database combines information on reported cases, outbreaks, associated mortality, and the country- and state-wise distribution of both vector and disease prevalence. All data have been carefully curated from NCVBDC, IDSP, and peer-reviewed literature, making it the first comprehensive resource of its kind in this field.
As part of the Wellcome Trust funded project
Title
Longitudinal characterization of clinico-epidemiological, genomic and immunological features of dengue and Zika infections and coinfections in Kerala, India: study protocol
Authors
Rahi, M., Rahul, A., Sharma, R., Saini, P., Shriram, A N., Rema Suresh, A., Thiruvengadam, K., Ramasamy, A., Raju, K H K., Veettilakath, J., Sugunan, S., Saheeda, T., Aravind, R., Chandele, A., Sharma, A., Anish, T S N.
Abstract
Introduction
The overlapping geographic distribution of dengue virus (DENV) and Zika virus (ZIKV), and their shared primary vector, facilitates co-circulation and coinfection or sequential infections in endemic regions. This overlap poses additional challenges due to immune cross-reactivity and the potential for altered or exacerbated clinical severity.
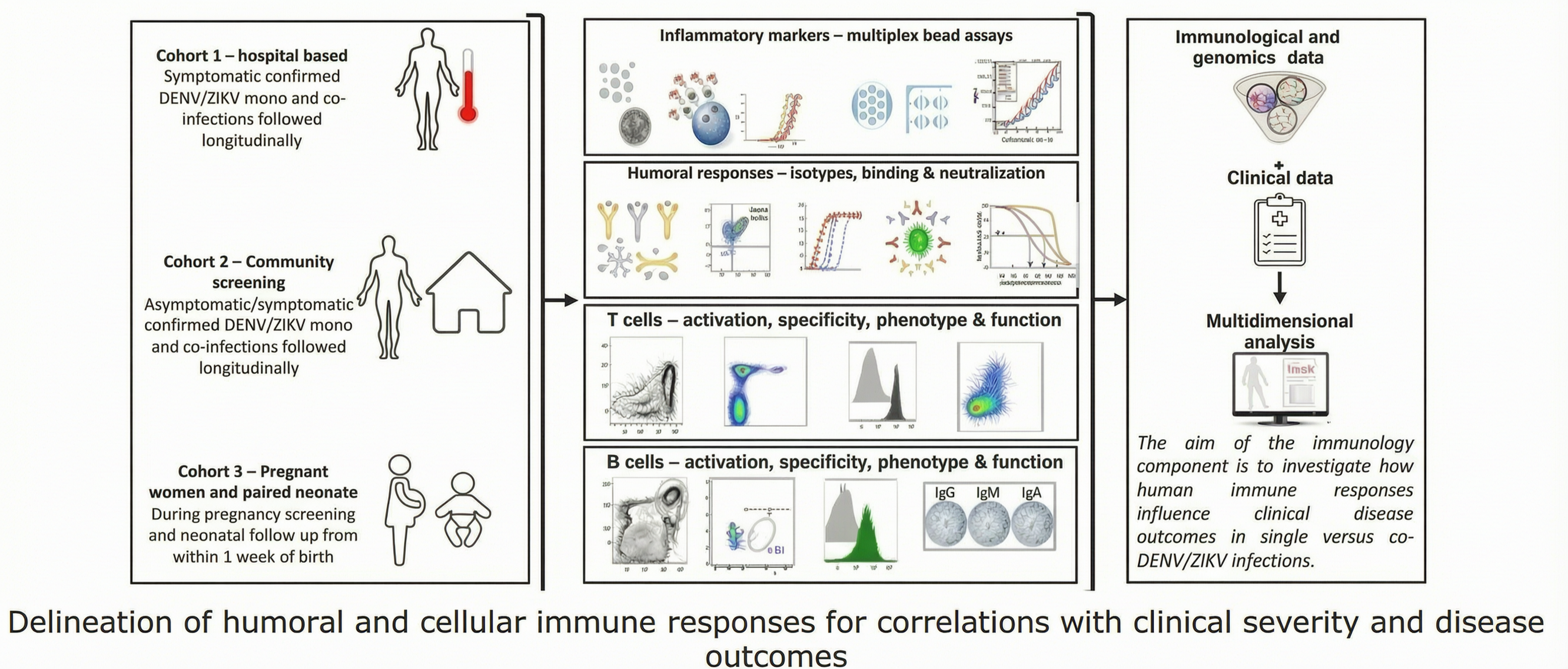
This study aims to estimate the burden of DENV-ZIKV infections and coinfections, characterise clinical and epidemiological profiles across adult, paediatric, and pregnant cohorts, assess viral genome diversity, and delineate humoral and cellular immune responses in relation to disease severity.
Kerala state in India, with robust surveillance, hyperendemic dengue transmission and documented ZIKV clusters, provides an ideal setting for this investigation.
Methods and Analysis
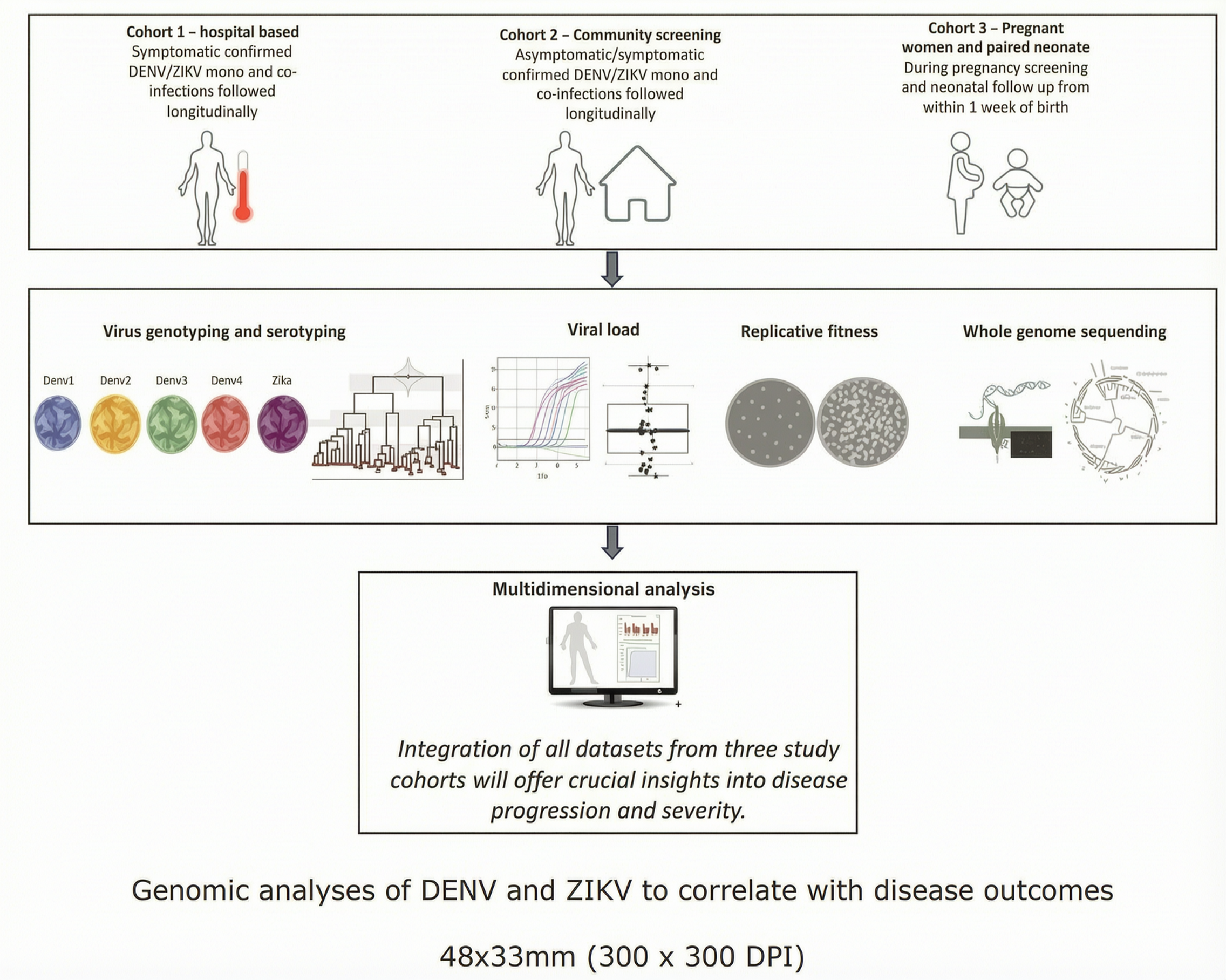
This longitudinal study will be conducted over a period of five years in the Thiruvananthapuram district of Kerala. Three cohorts comprising probable cases (~17,160 individuals), community clusters, and pregnant women (~10,400), along with their neonates, will be enrolled from public healthcare facilities.
Acute phase whole blood and/or plasma samples will be tested by RT-PCR for DENV and ZIKV, along with dengue serotyping and viral load quantification. Patients with confirmed infections will be followed longitudinally to evaluate clinical severity and disease outcomes.
Genomic characterisation will be performed using Nanopore whole-genome sequencing. Immune responses will be profiled using ELISAs, multicolour flow cytometry, and ELISpot assays.
Fortnightly surveillance of Aedes mosquitoes will be conducted in hotspot areas, combined with geospatial analyses. Multivariable regression and machine learning will be used to develop an integrative model to identify predictors of disease severity, adverse outcomes, and transmission risk.
Figures

Our Team

Dr. Amit Sharma
Team Lead
Dr. Syed Shah Areeb Hussain
Dashboard Designing

Dr. Pooja Rani Kuri
Analysis and Research

Pushparani Khwairakpam
Developer

Areeba Aziz
Data Collection

Anushka Dobhal
Data Collection

Prem Pandey
Data Collection
Contact Us
Contact Information
Address:
Dr Amit Sharma Lab,
Group Leader, Structural Parasitology, Molecular Medicine Group,
International Centre For Genetic Engineering And Biotechnology (ICGEB),
New Delhi, Delhi 110067
Tel: +91-11-26741358 | 26742360 | 26741361
Email Address: admin@chikdenzi.com